
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Introduction
Employer-sponsored benefits such as health insurance historically have been an important part of recruiting and retaining employees. However, as costs associated with health insurance rise, more employers are either changing the terms of their health insurance benefits to shift more of the premium burden on the employee, increasing deductibles and decreasing benefits, or ceasing to provide insurance at all.
The national average cost of health insurance increased by 119% during the last decade (The Kaiser Family Foundation and Health Research & Educational Trust, 2008). As the cost of this benefit increased, the proportion of employers, especially small employers, who could afford to offer insurance to their employees declined. Nationally, the percentage of employers with three to nine employees that offered health insurance declined from 57% to 49% between 2000 and 2008 (Napel, Bulchis, Trinity, et.al., 2008).
Additionally, the percentage of employees considered underinsured, including those who were offered plans with a deductible of $1,000 or more, increased from 16% to 35% during 2008 (Napel, Bulchis, Trinity, et.al., 2008). According to the U.S. Census Bureau, the percentage of Americans not covered by private or government health insurance rose from 12.9% in 1987 to 15.3% in 2007. People do not have insurance for a number of reasons. Sometimes their employer does not offer benefits, or they may be ineligible for other reasons. In other cases, an employee’s wages are not sufficient to afford the premiums (Kaiser Family Foundation, 2008). The number of uninsured employees will most likely continue to increase due to the current economic downturn and rising costs.
As a result of the growing number of uninsured people, hospitals shift costs to those who can pay by increasing the cost of services to insured patients, particularly those with employer-sponsored health insurance, to offset the loss in revenue. This causes insurance companies to increase premium costs to employers. An employer may require an employee to pay a larger share of the cost, or the employee may choose a plan with increased deductibles and co-pays and decreased benefits. Or, the employer may simply quit offering health insurance (Strengthening employer-based health care, 2009a).
A case study in New Jersey showed the percentage of uncompensated care, which includes charity care, bad debts, and the amount not paid by Medicare and Medicaid, increased by 4% in six years. However, the estimated cost of providing uncompensated care increased by 51% during the same time (Strengthening employer-based health care, 2009b). This rise in uncompensated care is occurring in Wyoming, too. According to officials at Wyoming Medical Center in Casper, the hospital has seen a 23% increase in the amount of uncompensated care between July 2008 and the present. They expect the amount of uncompensated care to be nearly $40 million by the end of the 2009 fiscal year (Rupp, 2009).
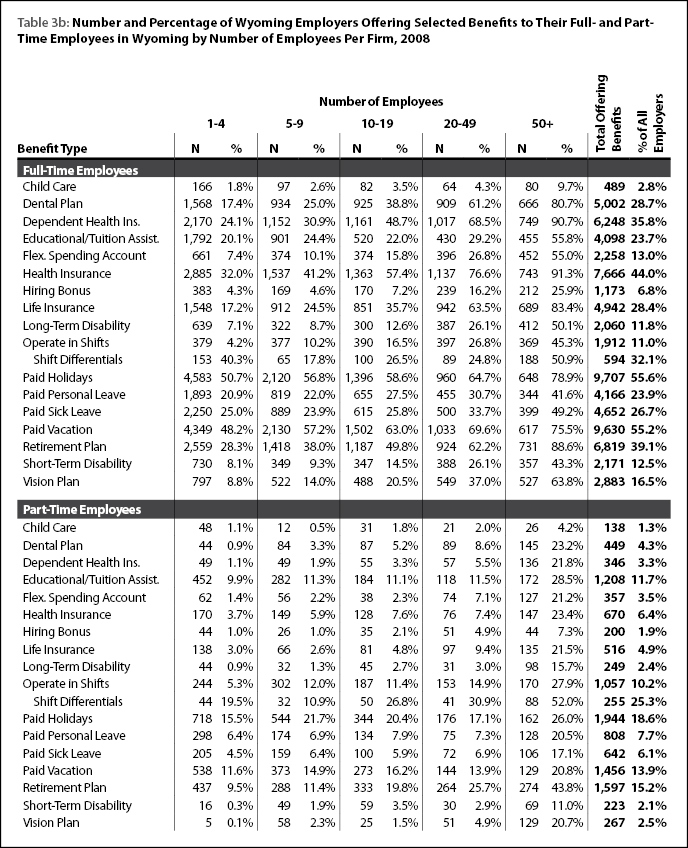
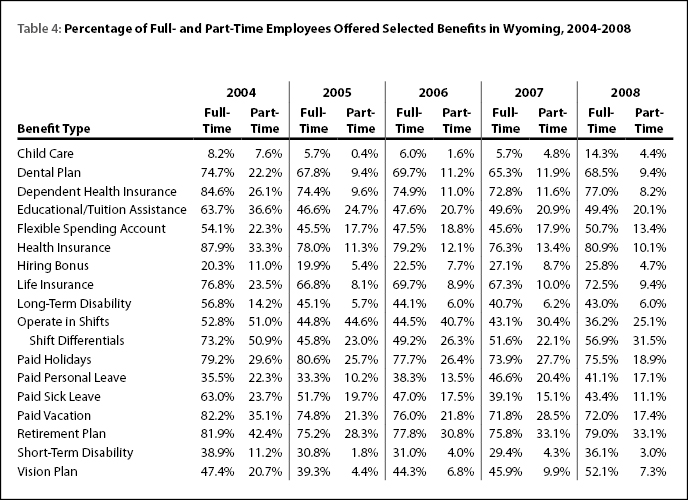
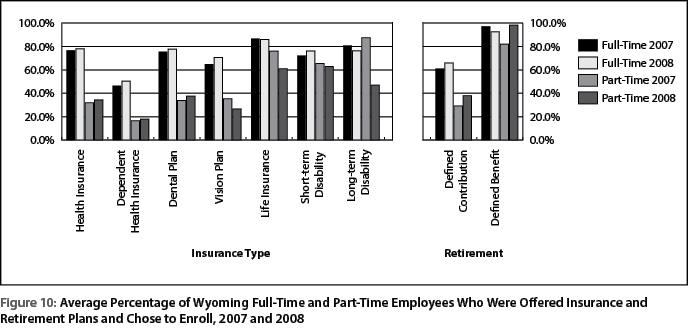
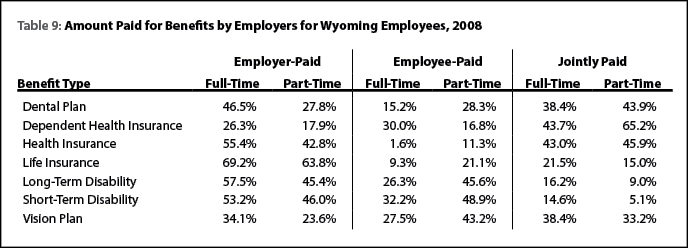
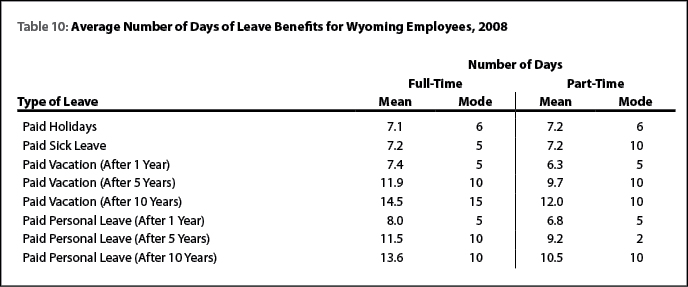
The purpose of the Wyoming Benefits Survey is three-fold. First, it provides a standard method of measuring how benefits are offered in the state. Second, it provides a means of monitoring trends over time and allows for a way of identifying major changes to the market and potential issues. Finally, it allows for research and policy analysis (Levit & Wiatrowski, 2001). The following analysis provides details of benefits in Wyoming during 2008.